Featuring insights from Mirjam Davidse and Quirijn Tummers
Thoracic surgery is entering a new era of precision. Earlier detection of lung cancer increasingly expands the possibilities for lung-sparing procedures. At the same time, detailed understanding of patient-specific anatomy may also allow more tissue-sparing approaches in selected complex or larger tumors, depending on their anatomical location. Together, these developments mean surgeons are more often faced with highly individualized decisions, balancing oncological certainty with the need to preserve as much healthy lung tissue and function as possible.
No two lungs are exactly alike. Pulmonary vessels, bronchial branching patterns, and segmental anatomy can vary substantially between patients, making surgical planning for lung resection highly complex. Especially in procedures where only a specific lung segment may be removed, a detailed understanding of patient-specific anatomy is critical for surgical precision, postoperative lung function, and ultimately patient quality of life. 1.2
A recent clinical research collaboration between the Netherlands Cancer Institute (NKI) and Thirona evaluated how advanced 3D lung visualization generated from AI-based anatomical segmentation could support surgical planning in early-stage lung cancer patients. Based on the perspectives of thoracic surgeon Quirijn Tummers and researcher Mirjam Davidse, this article explores how detailed anatomical reconstruction may improve understanding of segmental structures and increase confidence in surgical planning.
Lobectomy or segmentectomy? Balancing lung preservation with adequate tumor margins
For decades, lobectomy (removal of an entire lung lobe) has been the standard surgical approach for many lung cancer patients. Better understanding of patient-specific anatomy can help surgeons consider more tissue-sparing approaches such as segmentectomy, while still ensuring adequate oncological margins. 1
Unlike lobectomy, segmentectomy requires surgery within much smaller and anatomically complex boundaries. The procedure demands precise understanding of patient-specific vessels, bronchi, intersegmental planes, and tumor location to ensure adequate tumor margins while preserving as much functional lung tissue as possible.2.3.4
As Quirijn Tummers explains, the challenge is amplified by the large anatomical variation between patients. Although conventional CT already provides detailed anatomical information, surgeons still need to mentally reconstruct a three-dimensional understanding of these structures from cross-sectional images.
“The anatomical variation is huge in lung surgery. The more detailed you make a surgical procedure, the more important it becomes to understand this variation.”
(Quirijn Tummers, Thoracic Surgeon, NKI)
In practice, surgeons must answer several high-stakes questions during pre-operative planning:
- Is the tumor fully contained within the planned resection segment?
- Will the planned resection provide sufficient oncological margins?
- Which vessels and bronchi must be preserved?
- Can healthy lung tissue be spared without compromising surgical certainty?
These questions become particularly important in procedures where small lesions located deeper in the lung parenchyma may be neither directly visible nor palpable during surgery. In these cases, surgeons rely heavily on preoperative planning to determine whether the planned resection will fully contain the tumor while avoiding unnecessary removal of healthy tissue.
In this context, accurate visualization of inter-segmental planes is especially valuable, helping surgeons better understand the spatial relationship between tumors and surrounding anatomy before entering the operating room. 1
When additional anatomical insight could change the surgical plan
To better understand the clinical value of advanced 3D visualization in thoracic surgery planning, researchers at NKI retrospectively evaluated 25 early-stage lung cancer cases using conventional 2D CT imaging both with and without additional 3D anatomical reconstructions. Two experienced thoracic surgeons independently reviewed each case to assess whether the additional anatomical perspective influenced treatment planning decisions. In this workflow, Thirona’s LungQ® anatomical segmentation formed the foundation of the 3D visualization by delineating key structures such as lung segments, vessels, bronchi, and tumor-related anatomy.
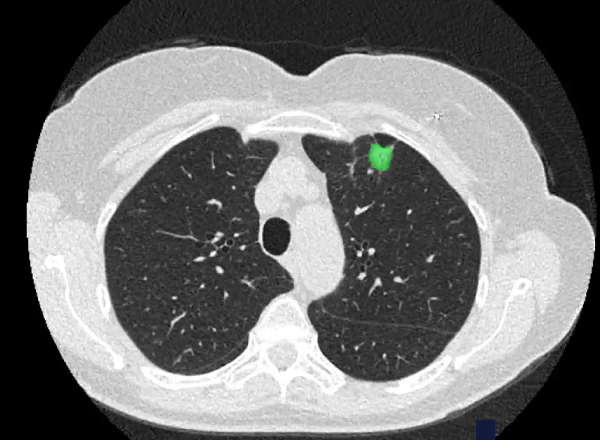
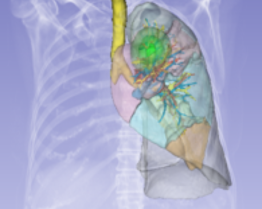
Left: CT scan showing the lung tumor
Right: AI-generated 3D lung model with precise lesion localization and planned resection margins (1 cm and 2 cm), alone with adjacent anatomical structures to support procedural planning
The impact on surgical planning was considerable. After reviewing the 3D visualizations, surgical plans changed in 34% of cases, substantially exceeding the predefined study threshold of 20%.
Most of these changes involved moving from lobectomy toward more tissue-sparing segmentectomy approaches. The added anatomical detail improved confidence in determining whether a tumor could safely be removed within a smaller resection area.
As Mirjam Davidse observed, one of the clearest findings was that 3D visualization improved surgeons’ assessment across all evaluated anatomical structures, with the largest gains seen for lung segments and oncological resection margins – areas that are particularly important when planning segmentectomies.
Importantly, the value of the 3D models was not limited to better visualization alone. The reconstructions helped surgeons develop a more intuitive spatial understanding of how tumors relate to surrounding anatomy and segmental boundaries – information that can be difficult to fully interpret from cross-sectional CT slices alone.
“A detailed 3D reconstruction provides greater confidence that the planned resection will achieve sufficient margins while preserving healthy lung tissue.”
(Quirijn Tummers, Thoracic Surgeon, NKI)
This additional anatomical perspective appeared particularly valuable in minimally invasive procedures involving smaller lesions located deeper within the lung tissue. In such cases, the participating clinicians explained that the surgical strategy depends heavily on accurate preoperative anatomical assessment, as tumors may not be directly visible during the intervention itself.
Beyond influencing the planned extent of resection, the study also showed a significant increase in surgeon confidence scores after reviewing the 3D visualizations. The research team suggests that detailed anatomical reconstruction may help reduce uncertainty during planning of anatomically complex lung resections, particularly in cases where multiple surgical approaches could be considered.
Looking ahead: Supporting more lung-sparing surgery for patients
While the study demonstrated how lung resection planning can benefit from 3D visualization of patient-specific anatomy, it also points to a broader direction in thoracic surgery: using AI-generated anatomical insight to support more personalized surgical decisions. As minimally invasive and robotic-assisted thoracic surgery continue to evolve, the ability to visualize each patient’s bronchial, vascular, and segmental anatomy may help surgeons better assess which approach is feasible, with the aim of preserving more healthy lung tissue and supporting better outcomes for patients.

This level of anatomical understanding may also strengthen communication with patients. As Quirijn Tummers noted, a 3D model can make it easier to explain what will happen during surgery, helping patients better understand the treatment strategy and planned procedure than when looking at difficult-to-interpret 2D CT images alone.
In that sense, 3D visualization could become more than an additional view of CT data. It may act as an important practical bridge between imaging and surgery, translating complex anatomy into a clearer surgical roadmap, particularly when different resection strategies are being assessed.
“The surgeon is responsible for what he does to the patient. But the model has to be robust enough.”
(Quirijn Tummers, Thoracic Surgeon, NKI)
Over time, this potential could even extend beyond preoperative planning, with patient-specific 3D models supporting intraoperative orientation by helping surgeons compare the planned anatomy with what they see during the procedure. Tummers and his team envision a future where such models could be available directly in the surgical environment, supporting orientation during complex resections.
At the same time, broader clinical use depends on reliability. As Tummers emphasized: “The surgeon is responsible for what he does to the patient. But the model has to be robust enough.”
In practice, this means distinguishing between anatomical details that are helpful and those that are clinically decisive. As Tummers explained, minor inaccuracies in very small distal vessel branches may not necessarily affect the procedure, but the core structures guiding the resection, including intersegmental planes and key vascular and bronchial anatomy, must be reliable.
This is where extensively validated anatomical segmentation becomes essential. As Mirjam Davidse emphasized, clinical implementation will depend not only on the clinical value of 3D models, but also on workflow efficiency, reliability, and the ability to generate reconstructions with minimal manual interaction. When built on thoroughly validated lung analysis technology, AI-based segmentation can form a solid foundation for thoracic surgery that is more precise, more personalized, and focused on preserving patient lung function.
- Miao et al; Artificial Intelligence–Driven Three-Dimensional Reconstruction in Lung Cancer Surgery: Current Status and Future Perspectives, Artificial Intelligence–Driven Three‐Dimensional Reconstruction in Lung Cancer Surgery: Current Status and Future Perspectives – Miao – ANZ Journal of Surgery – Wiley Online Library
- Xu et al; The impact of segmentectomy versus lobectomy on pulmonary function in patients with non-small-cell lung cancer: a meta-analysis, Journal of Cardiothorac Surgery The impact of segmentectomy versus lobectomy on pulmonary function in patients with non-small-cell lung cancer: a meta-analysis – PMC
- Laven et al; Advancements in 3D lung models for minimally invasive lung cancer surgery: from static to real-time dynamic modeling, Advancements in 3D lung models for minimally invasive lung cancer surgery: from static to real-time dynamic modeling – Laven – Translational Lung Cancer Research
- Quinten J et al; Artificial intelligence-based pulmonary vessel segmentation: an opportunity for automated three-dimensional planning of lung segmentectomy, Artificial intelligence-based pulmonary vessel segmentation: an opportunity for automated three-dimensional planning of lung segmentectomy